


Leveling as a difference maker in clinical psychology
Income inequality has pernicious effects on well-being. Still, it does not seem to have had a tremendous backlash in the field of clinical psychology. Should it?
‘We cannot succeed when a shrinking few do very well and a growing many barely make it’
- Barack Obama in his Inaugural speech (January 20th 2013, Washington)
A key task for clinical psychology is to find those variables that make the difference between ‘non-clinical vs. clinical behavior’ (i.e. difference makers). Well established difference makers are stressors, ranging from exposure to traumatic events in childhood (e.g. being abused) to stressful events that occur in adulthood such as being fired, a divorce, or maybe even worse, having a very bad marriage. Having a poor physical health and personality traits such as being a perfectionist or a neurotic also add as a weight in the equation. Plus, there is the awareness that biology might make a difference as well (e.g. genetic vulnerabilities). Apparently, the set of difference makers is broad and reaches far. Still, together they often do not provide 100% satisfaction in explaining how clinical behavior comes about. What possibly could or needs to be added? Maybe, clinical psychology should listen to the epidemiologists Wilkinson and Pickett because they have a story to tell.
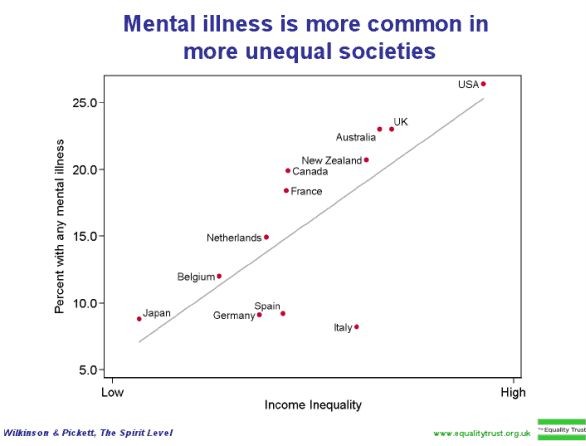
The story of Wilkinson and Pickett is as simple as it is striking. They show that those societies that have the broadest differences in incomes do absolutely worst with regard to mental health. The figure tells it all - the percentage of persons with a mental illness increases from 6 percent in the most equal society to as much as 25 percent in the most unequal society. Similar findings have been reported on a great deal of indices of well-being (e.g. trust and substance dependency). One explanation is that persons are sensible to social status and that negative comparisons may lead to disappointment, to grief, and yes, even to mental illness. Another is that the more equal a society is the more likely it is are to act for the common good. This explanation fits with the notion that the percentage of persons with mental illness in less equal societies is higher in both the 20% top and 20% bottom income groups. Important here is that differences in the prevalence of mental illness are not evident as a function of absolute wealth of a society. Conclusion: income inequality has pernicious effects on well-being.
Still, income inequality does not seem to have had a tremendous backlash in the field of clinical psychology. Should it? On the one hand, if it adds to your model of what causes ‘non-clinical vs. clinical behavior’ then why not. Because, if you can build a model of a clinical behavior, for instance depression, you may be close to understand it, to treat it, and to add to the well–being of many. However, social or income inequality is different from the many other difference makers in clinical psychology in that it needs an inter-disciplinary approach to understand (e.g. political science and philosophy, and sociology) and above all a fair amount of societal discussion.
For more information see the article Equality, sustainability, and quality of life, BMJ (2010). And this TED Talk by Wilkinson: 'How economic inequality harms societies' (~16 minutes):


